- Visibility 53 Views
- Downloads 24 Downloads
- DOI 10.18231/j.ijooo.2024.040
-
CrossMark

Orbital trauma mimicking globe rupture: A case report of preserved vision
- Author Details:
-
Suchitra Dash
-
Sarita Panda
-
 Piyush Jain *
Piyush Jain *
-
Ankita Mishra
-
Deepika Priyadarshini
-
Radhakanta Bhoi
Introduction
Ocular penetrating and perforating injuries, commonly referred to as open globe injuries, can lead to severe vision loss or even the loss of the eye. Penetrating injuries occur when a sharp object lacerates the eye, causing an entry wound without creating an exit wound.[1] About 40% of these injuries are complicated by the presence of an intraocular foreign body (IOFB), which can be either toxic (such as iron, copper, or vegetable matter) or inert (such as glass or plastic). Vision loss may result not only from the mechanical damage caused by the foreign object but also from complications like endophthalmitis, retinal detachment, metal toxicity, or sympathetic ophthalmia.
Epidemiological studies highlight that male gender is a significant risk factor for ocular trauma.[2], [3] In one retrospective study, retinal detachment was observed in 29% of open globe injuries. Early diagnosis, prompt referral, removal of the foreign body, and surgical repair are essential for preserving both visual acuity and the integrity of the eye.
Case Report
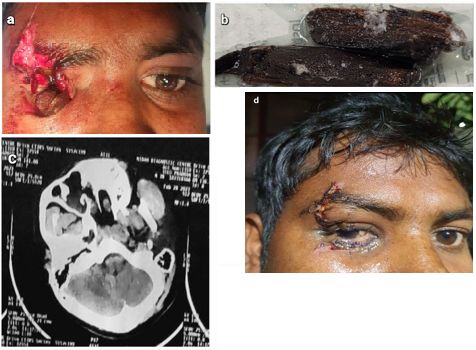
A 38-year-old male presented to our emergency with a history of trauma to the right eye by a wooden object. Examination revealed an extensive laceration involving the eyebrow, eyelid, and periorbital ecchymosis with subconjunctival haemorrhage. A wooden foreign body was visible within the right orbit ([Figure 1]a). Visual acuity was not assessed initially.
A CT scan demonstrated a radiolucent foreign body in the medial aspect of the right extraconal region along with a right globe rupture ([Figure 1]c). Additionally, fractures of the floor, medial wall, and lamina papyracea of the right orbit were identified, along with bilateral maxillary hemosinusitis. B-scan ultrasonography revealed an attached retina and anechoic vitreous.
Treatment
Considering the CT scan findings, Fortunately, despite this on OT table patient’s injury was completely extraconal with an intact right eyeball and his vision was preserved after the surgery, a remarkable outcome. ENT surgeon was called due to maxillary hemosinus as per the CT report but luckily, there was no bleeding during the surgery, as was highly probably. Furthermore, during the recovery, there were no complications like RAPD, EOM injury, retinal detachment, or vitreous haemorrhage, which was also a miraculous positive outcome. The wooden foreign body was successfully removed from the right extraconal space, and the eyelid laceration was repaired. Post-operatively, the patient received broad-spectrum antibiotics, analgesics, corticosteroids, and topical ophthalmic medications with a steroid taper.
Outcome
At 10 days post-surgery (POD-10), the patient’s best-corrected visual acuity (BCVA) was 6/9, indicating significant vision ([Figure 1]d). The steroid medication was tapered, and the patient recovered without complications such as restricted ocular motility (RAPD), extra ocular muscle injury (EOM), retinal detachment, or vitreous hemorrhage.
Discussion
Wooden IOFBs can cause a rapidly healing wound at the surface, leaving residual foreign material in the wound and inducing subsequent.[4] As a general rule, a fresh IOFB should not be left in the eye after open-globe injury. However, if the IOFB is verifiable inert, and no signs of endophthalmitis was observed, early surgery should be considered carefully for its risk of potential complications may possibly bring more damage to the eye than the IOFB itself. In cases of posterior segment IOFBs, a decision of vitrectomy or not must be made in time: the more severe tissue damage is, the more indication of vitrectomy is given to remove the IOFB and prevent subsequent damage to the intraocular structure.[5]
Accurate localization is necessary preoperatively. CT scan accurately localizes it in the ocular coat, anterior segment, posterior segment, or extra ocular locations.[6]
Conclusion
This case report underscores the significance of meticulous clinical and radiological assessment in cases of orbital trauma, especially when imaging raises concerns about globe rupture. The successful preservation of vision in this case, despite initial alarming findings, highlights the importance of correlating imaging results with clinical evaluation to avoid unnecessary surgical interventions. [7]
The management of foreign bodies in the orbit demands a high index of suspicion for associated complications, including endophthalmitis, retinal detachment, and extraocular muscle injury. In this case, a multidisciplinary approach involving ophthalmology and ENT specialists, combined with timely surgical exploration and removal of the foreign body, ensured an excellent functional outcome with no post-operative complications.[8]
Furthermore, this case illustrates the challenges posed by wooden intraorbital foreign bodies, which can mimic severe ocular injuries due to their radiolucent nature. It reinforces the value of modern imaging techniques, such as CT scans and B-scan ultrasonography, for accurate localization and diagnosis.
Finally, this report serves as a reminder that early intervention, postoperative care with antibiotics and corticosteroids, and vigilant follow-up are essential in managing orbital trauma effectively. Such cases emphasize the need for ophthalmologists to maintain a balanced approach—acting decisively while avoiding overly aggressive procedures that may compromise visual outcomes.
Conflicts of Interest
There are no conflicts of interest.
Source of Funding
None.
References
- F Kuhn, R Morris, C D Witherspoon. A standardized classification of ocular trauma. Graefes Arch Clin Exp Ophthalmol 1996. [Google Scholar]
- DR May, FP Kuhn. The epidemiology of serious eye injuries from the United States Eye Injury Registry. Graefes Arch Clin Exp Ophthalmol 2000. [Google Scholar]
- TP Stryjewski, CM Andreoli, D Eliott. Retinal detachment after open globe injury. Ophthalmology 2014. [Google Scholar]
- DW Parke, HW Flynn, YL Fisher. Management of intraocular foreign bodies: A clinical flight plan. Can J Ophthalmol 2013. [Google Scholar]
- D Loporchio, L Mukkamala, K Gorukanti, M Zarbin, P Langer, N Bhagat. Intraocular foreign bodies: A review. Surv Ophthalmol 2016. [Google Scholar]
- Y Qi, FY Zhang, GH Peng, Y Zhu, GM Wan, WZ Wang. Characteristics and visual outcomes of patients hospitalized for ocular trauma in central China: 2006-2011. Int J Ophthalmol 2015. [Google Scholar]
- SJ Ryan. Traction retinal detachment. XLIX Edward Jackson Memorial Lecture. Am J Ophthalmol 1993. [Google Scholar]
- AJ Rong, KC Fan, B Golshani, M Bobinski, JP Mcgahan, D Eliott. Multimodal imaging features of intraocular foreign bodies. Semin Ophthalmol 2019. [Google Scholar]